

DDH is one of the most common congenital conditions and according to the International Hip Dysplasia Institute, around one in 20 full-term babies have a degree of hip instability and between two to three in every 1,000 infants will require medical treatment.
Despite the prevalence of the condition, information is scarce and support scant. When my son was diagnosed six years ago all I found were horror stories and awful images when all I wanted were the facts.
The facts, incase you are wondering, go a little something like this:
DDH occurs when the ball and socket hip joint fails to develop correctly and whilst it isn’t life threatening, it certainly is life changing and that has been the case for my family.
The ball is called the “femoral head” and is at the top of the femur or thighbone. The socket is called the “acetabulum” and this is a part of the pelvis. Ligaments, muscles and a joint capsule hold them together and promote growth and strength.
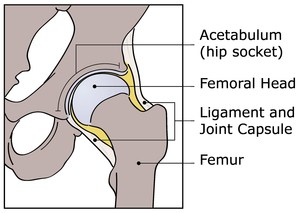
In a normal, healthy hip, the head of the femur is smooth and round and the acetabulum is a smooth cup-like shape and the two sit together like an egg in an egg-cup.
DDH occurs when the two don’t fit snugly together.
There are various degrees of DDH severity and I think that it is pretty fair to say that no two cases are ever the same and this can be one of the hardest things about this condition.
The main elements for parents, and health professionals, to be aware of are:
- If the ball is not held in place securely this can indicate a shallower than average socket; this is called acetabular dysplasia
- A shallow socket can create an unstable joint which means the ball may slide in and out of the socket, this is called a dislocatable or subluxatable hip
- If the ball simply has no contact with the socket and stays outside the joint, it is called a dislocated hip
In the majority of cases there is no clear, identified cause or risk and even the most qualified medical professionals cannot predict DDH and do not known why a baby develops the condition.
We do however know that statistically DDH is more common in:
- A baby born in the breech position
- A baby who was breech in the last three months of pregnancy
- A family history of DDH (Lucas but there was STILL a late diagnosis)
- First pregnancies
- Baby girls
- If there is a deficiency of amniotic fluid in the womb
- Babies with tortorticollis, a tightness of the muscles on one side of the neck
- Babies with a mild foot abnormality
For some children, those found earlier enough, a soft harness (Pavlik harness) can correct the situation. For others, like my son Lucas, surgery is necessary.
There are several places on line, such as Groupon, where you can find necessary items for post DDH surgery. Be sure to have all of your ducks in a row before you head out to hospital – and your trip home may be a bit easier.
I was left floundering to navigate the murky waters of DDH six years ago and I hope that the writing on my blog, and the launch of my book Cast Life, will make things a little bit easier.
As well as looking at the medical details of DDH and treatments, this book also looks at the emotional issues. It contails comments from experts as well as parents and real life case studies show that however hard life with DDH might seem, you can do it.
If you think your child may have DDH or know a family on their journey, please flag this post as moving forward there is now help out there.
Natalie